Stroke also known as cerebrovascular accident ,is a sudden impairment of cerebral circulation in one or more of the blood vessels supplying the brain,it interrupts or diminishes the blood supply ,causing necrosis in brain tissues.the sooner circulation returns to normal after the stroke ,the better chances of complete recovery .about ½ of those who survive remains permanently disabled and suffer another stroke within weeks, months or years. Major causes of stroke include thrombosis, embolism and hemorrhage.

Thrombosis is the most common cause of in middle aged and elderly people.its usually result from an obstruction in the extra- cerebral vessels,but sometimes it's intracrebral. The risks increases with obesity,smoking,hormonal contraceptive use and surgery.
Emboli stroke is the second most common cause of stroke. Embolism is a blood vessel occlusion caused by fragmented clot,a tumor,fat,bacteria,or air. It can occur at any age especially in patients with a history of rheumatic heart disease,endocarditis,post traumatic valvular disease, and cardiac arrhythmias. It also occur after open heart surgery ,embolism usually develops rapidly in 10 to 20 sec and without warnings he left middle cerebral artery is the embolic site.
Hemorrhage is the third most common cause of stroke,may also suddenly occur at any age. It rises from chronic hypertension or aneurysms which cause a sudden rupture of cerebral artery. Increase in cocaine use by youngsters leads to hemorrhagic stroke due severe hypertension caused by the drug.
Factors increase the risk of stroke include.
- History of transient ischemic attack
- Atherosclerosis
- Hypertension
- Arrhythmias special atrial fibrillation
- Rheumatic heart disease
- DM
- Gout
- Orthostatic hypotension
- High serum triglyceride levels
- Lack of exercise
- Hormonal contraceptive use
- Drug abuse
- Smoking
- Family history of cerebrovascular disease
- Sickle cell disease
Clinical features
In stroke function loss reflects damage to the brain area normally by occluded or rupture artery.one patient may experience only mild weakness ,another may develop uni lateral paralysis.hypoxia and ischemia produce edema that affects distal parts of the brain.
Middle cerebral artery
- Aphasia/dysphasia
- Reading problems
- Inability to write
- Visual field cuts
- Hemiparesis on the affected side.
- Internal caryatid artery
- Numbness
- Paralysis
- Weakness
- Headache
- Sensory changes
Anterior cerebral artery
- Confusion
- Weakness
- Incontinence
- Poor coordination
- Impaired motor and sensory functions
- Personal changes
Vertebral or bacillary artery
- Mouth and lip numbness
- Dizziness
- Vision deficits,colour blindness
- Poor coordination
- Dysphagia
- Slurred speech
Posterior cerebral artery
- Visual field cuts
- Sensory impairment
- Coma
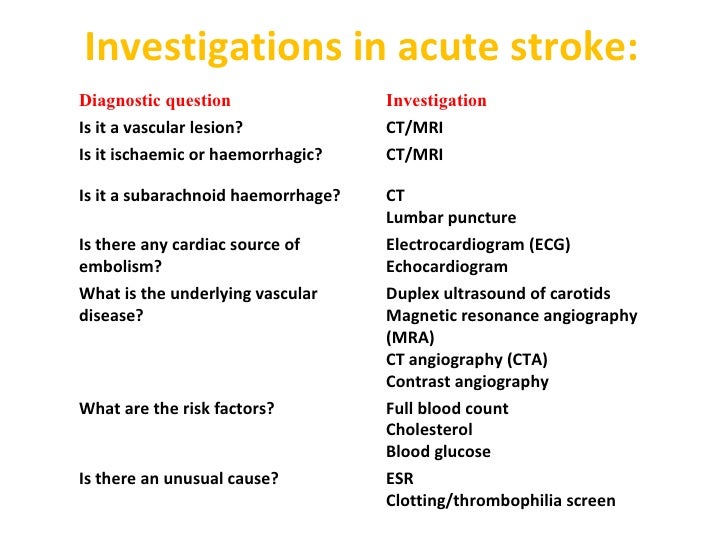
Investigation
 Medical Management and all you need to know about STROKE
Medical Management and all you need to know about STROKE
Management
Acute Ischemic Stroke
Hemorrhagic stroke
Acute Ischemic Stroke
- Assess airway, breathing and circulation
- Monitor cardiac activity for the first 24 hours
- Fibrinolytic therapy- IV administration of rtPA (recombinant tissue plasminogen activator)- for patients who are hypertensive before initiating fibrinolytic therapy. (<185mmHg systole and <110mmHg diastole) (
- Ventilatory support
- Supplemental oxygen
- Antipyretics (Acetaminophen)- to prevent hyperthermic accelerated brain damage
- IV insulin - for hyperglycemia in acute ischemic stroke in the first 24 hours
- Intra-arterial reperfusion by thrombectomy
- Aspirin 325mg oral 24-48 hours
- Antihypertensives- Calcium channel blockers
- Mannitol to reduce ICP
- Vasodilators- Sodium nitroprusside
- Neuroprotective agents
Hemorrhagic stroke
- Assess airway, breathing and circulation
- Monitor cardiac activity
- Endotracheal intubation
- Anticonvulsants
- Antihypertensives (beta-blockers and ACEI)
- Elevate head of bed to around 30 degrees (for better jugular venous blood flow)
- Antacids
- Mannitol
- Analgesics
- Reversal therapy- IV vitamin K, prothrombin complex concentratio, fresh frozen plasma and rFVIIa (Liebeskind 2015)
- Endovascular embolization therapy
- Ventriculostomy (Liebeskind 2015)
References
- Adams RJ, et al. (2003). Coronary risk evaluation in patients with transient ischemic attack and ischemic stroke: A scientific statement for healthcare professionals from the Stroke Council and the Council on Clinical Cardiology of the American Heart Association/American Stroke Association. Circulation, 108(10): 1278–1290. Also available online: http://circ.ahajournals.org/content/108/10/1278.full.
- Brott TG, et al. (2010). Stenting versus endarterectomy for treatment of carotid-artery stenosis. New England Journal of Medicine, 363(1): 11–23.
- Ederle J, et al. (2009). Randomized controlled trials comparing endarterectomy and endovascular treatment for carotid artery stenosis: A Cochrane systematic review. Stroke, 40(4): 1373–1380.
- Goldstein LB, et al. (2010). Guidelines for the primary prevention of stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. Published online December 2, 2010 (doi: 10.1161/STR.0b013e3181fcb238). Also available online: http://stroke.ahajournals.org/content/42/2/517.full.
- Guyatt GH, et al. (2012). Executive summary: Antithrombotic therapy and prevention of thrombosis, 9th ed.—American College of Chest Physicians evidence-based clinical practice guidelines. Chest, 141(2, Suppl): 7S–47S.
- Lansberg MG, et al. (2012). Antithrombotic and thrombolytic therapy for ischemic stroke. Antithrombotic therapy and prevention of thrombosis, 9th ed. American College of Chest Physicians evidence-based clinical practice guidelines. Chest, 141(2, Suppl): e601S–e636S. Also available online: http://journal.publications.chestnet.org/article.aspx?articleid=1159534.
- Latchaw RE, et al. (2003). Guidelines and recommendations for perfusion imaging in cerebral ischemia: A scientific statement for healthcare professionals by the writing group on perfusion imaging, from the Council on Cardiovascular Radiology of the American Heart Association. Stroke, 34(4): 1084–1104. Also available online: http://stroke.ahajournals.org/content/34/4/1084.full.
- Morgenstern LB, et al. (2010). Guidelines for the management of spontaneous intracerebral hemorrhage. Stroke, 41(9): 2108–2129. Also available online: http://stroke.ahajournals.org/content/41/9/2108.full.
- Skinner JS, Cooper A (2011). Secondary prevention of ischaemic cardiac events, search date May 2010. BMJ Clinical Evidence. Available online: http://www.clinicalevidence.com.
- Smith SC, et al. (2011). AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: A guideline from the American Heart Association and American College of Cardiology Foundation. Circulation, 124(22): 2458–2473. Also available online: http://circ.ahajournals.org/content/124/22/2458.full.
- Spence JD, et al. (2010). Effects of intensive medical therapy on microemboli and cardiovascular risk in asymptomatic carotid stenosis. Archives of Neurology, 67(2): 180–186.
- U.S. Preventive Services Task Force (2007). Screening for carotid artery stenosis. Available online: http://www.ahrq.gov/clinic/uspstf/uspsacas.htm.
- Wahlgren N, et al. (2008). Thrombolysis with alteplase 3-4.5 h after acute ischemic stroke (SITS-ISTR): An observational study. Lancet. Published online September 15, 2008
No comments:
Post a Comment