Heart failure is defined as an inability of the heart to deliver blood at a rate required by metabolising tissues despite normal filling pressures.

CARDIAC HAEMODYNAMICS
Cardiac Output (CO) is the volume of blood expelled by the ventricles in a minute. Its around 5 – 7 litres although in LVF this will be reduced.
Factors determine cardiac output
Preload: the pressure that fills the ventricles during diastole(when the ventriles relax)
Afterload: resistance to flow in the arterial tree against which the heart must work.
Contractility: refers to the muscular pumping ability of the ventricles.
CAUSES OF ACUTE LVF
· Volume overload
· Drugs e.g. beta blockers, cocaine
· Infection e.g. Myocarditis
· Ischaemic Heat Disease / Myocardial Infarction
· Hypertension
· Aortic Stenosis
· Pathophysiology
In LVF the cardiac output is reduced e.g. secondary to an acute Myocardial Infarction. Failure of the ventricles to eject blood results in increased intracardiac pressures and pulmonary capillary pressure.
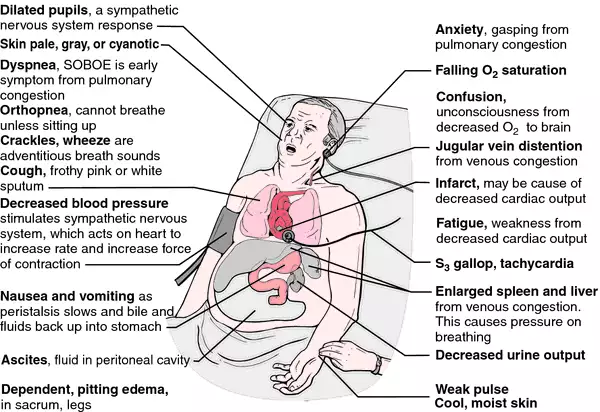
CLINICAL PRESENTATION
· Cough
· Crepitations - after coughing
· Hypoxia & cyanosis
· Sweating
· Tachycardia
· Fatigue / reduced exercise tolerance
· Dyspnoea
· Frank pulmonary oedema
· Paroxysmal nocturnal dyspnoea
Investigations

Following can be identifeid therough x-ray
· An enlarged heart
· the lungs will appear whiter often with a typical ‘bats wing’ distribution of oedema
· Dilated pulmonary capillaries and upper lobe diversion
Endomyocardial biopsy- recommended test to be carried out if the patient has deteriorating clinical HF despite appropriate treatment
Cardiopulmonary stress test- to test the patient's functional capacity (6 minute walk which evaluate factors such as distance, dyspnea index and the patient's vital sign changes)
Complete blood count (CBC)- to determine cause of HF
Urinalysis
Coronary arteriography
Doppler ultrasound scan
Cardiac MRI
Left-sided cardiac catheterization and coronary angiography- used when the cause of HF cannot be determined using other methods
Serum electrolytes- can be affected due to fluid shifts
BUN and serum creatinine- confirm reduced kidney perfusion
Fasting blood sugar
Liver function test- evaluate the effect of HF on the liver
BNP levels which will rise due to H
MANAGEMENT
Immediate management consists of :
Morphine IV as required Inoder to relive anxiety but may also reduce preload and afterload Oxygen
Supplemental oxygen- noninvasive positive pressure ventilation (NIPPV)
Drug therapy:
Diuretics: help by reducing circulatory volume and thereby reducing preload. An intravenous loop diuretic such as Frusemide is administered in the first instance
Venodilators: an intravenous infusion of Glceryl Trinitrate may be useful in reducing preload and afterload and may also improve coronary blood flow. Caution must be exercised in patients who are hypotensive
Inotropic drugs: these drugs are used to increase myocardial contractility and output. They are often classified according to their activity at alpha and beta receptors.
Drugs with mainly alpha activity will:
· increase afterload
· increase blood pressure
· slow pulse rate
Drugs with mainly beta activity will:
· reduce afterload
· increase pulse rate and cardiac output
Dobutamine (Dobutrex)
Exerts its effects on beta1 and beta 2 receptors and thereby Increases myocardial contractility and output. It has no renal (dopaminergic) effects.
The standard dose is 2.5 - 20 micrograms per KG per minute by continuous intravenous infusion
Dobutamine does exert chronotropic effects and it may increase myocardial oxygen consumption and aggravate angina
Side effects include:
· ventricular arrhythmias tachycardia
· hypokalaemia
· Angina
Implantation of cardioverterdefibrilators and coronary artery bypass graft.
References
CARDIAC HAEMODYNAMICS
Cardiac Output (CO) is the volume of blood expelled by the ventricles in a minute. Its around 5 – 7 litres although in LVF this will be reduced.
Factors determine cardiac output
Preload: the pressure that fills the ventricles during diastole(when the ventriles relax)
Afterload: resistance to flow in the arterial tree against which the heart must work.
Contractility: refers to the muscular pumping ability of the ventricles.
CAUSES OF ACUTE LVF
· Volume overload
· Drugs e.g. beta blockers, cocaine
· Infection e.g. Myocarditis
· Ischaemic Heat Disease / Myocardial Infarction
· Hypertension
· Aortic Stenosis
· Pathophysiology
In LVF the cardiac output is reduced e.g. secondary to an acute Myocardial Infarction. Failure of the ventricles to eject blood results in increased intracardiac pressures and pulmonary capillary pressure.
CLINICAL PRESENTATION
· Cough
· Crepitations - after coughing
· Hypoxia & cyanosis
· Sweating
· Tachycardia
· Fatigue / reduced exercise tolerance
· Dyspnoea
· Frank pulmonary oedema
· Paroxysmal nocturnal dyspnoea
Investigations

Following can be identifeid therough x-ray
· An enlarged heart
· the lungs will appear whiter often with a typical ‘bats wing’ distribution of oedema
· Dilated pulmonary capillaries and upper lobe diversion
Endomyocardial biopsy- recommended test to be carried out if the patient has deteriorating clinical HF despite appropriate treatment
Cardiopulmonary stress test- to test the patient's functional capacity (6 minute walk which evaluate factors such as distance, dyspnea index and the patient's vital sign changes)
Complete blood count (CBC)- to determine cause of HF
Urinalysis
Coronary arteriography
Doppler ultrasound scan
Cardiac MRI
Left-sided cardiac catheterization and coronary angiography- used when the cause of HF cannot be determined using other methods
Serum electrolytes- can be affected due to fluid shifts
BUN and serum creatinine- confirm reduced kidney perfusion
Fasting blood sugar
Liver function test- evaluate the effect of HF on the liver
BNP levels which will rise due to H
MANAGEMENT
Immediate management consists of :
Morphine IV as required Inoder to relive anxiety but may also reduce preload and afterload Oxygen
Supplemental oxygen- noninvasive positive pressure ventilation (NIPPV)
Drug therapy:
Diuretics: help by reducing circulatory volume and thereby reducing preload. An intravenous loop diuretic such as Frusemide is administered in the first instance
Venodilators: an intravenous infusion of Glceryl Trinitrate may be useful in reducing preload and afterload and may also improve coronary blood flow. Caution must be exercised in patients who are hypotensive
Inotropic drugs: these drugs are used to increase myocardial contractility and output. They are often classified according to their activity at alpha and beta receptors.
Drugs with mainly alpha activity will:
· increase afterload
· increase blood pressure
· slow pulse rate
Drugs with mainly beta activity will:
· reduce afterload
· increase pulse rate and cardiac output
Dobutamine (Dobutrex)
Exerts its effects on beta1 and beta 2 receptors and thereby Increases myocardial contractility and output. It has no renal (dopaminergic) effects.
The standard dose is 2.5 - 20 micrograms per KG per minute by continuous intravenous infusion
Dobutamine does exert chronotropic effects and it may increase myocardial oxygen consumption and aggravate angina
Side effects include:
· ventricular arrhythmias tachycardia
· hypokalaemia
· Angina
Implantation of cardioverterdefibrilators and coronary artery bypass graft.
References
- American Heart Association. Classes of heart failure. Available athttp://www.heart.org/HEARTORG/Conditions/HeartFailure/AboutHeartFailure/Classes-of-Heart-Failure_UCM_306328_Article.jsp. Accessed September 6, 2011.
- [Guideline] Hunt SA, for the Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. Sep 20 2005;46(6):e1-82.
- [Guideline] Dickstein K, Cohen-Solal A, Filippatos G, et al. for the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J. Oct 2008;29(19):2388-442.
- [Guideline] Lindenfeld J, Albert NM, Boehmer JP, et al, for the Heart Failure Society of America. Executive summary: HFSA 2010 comprehensive heart failure practice guideline. J Card Fail. Jun 2010;16(6):e1-194.
No comments:
Post a Comment